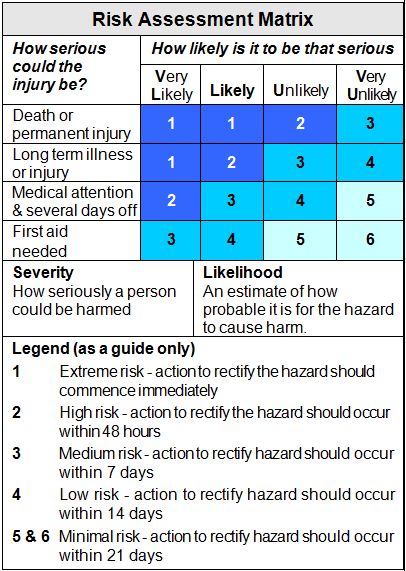
FacebookThis field is for validation purposes and should be left unchanged.Type of hazard Near Miss Workplace Hazard Hazardous Work Practice Time and date of incidentTime : Hours Minutes AM PM AM/PM Date DD slash MM slash YYYY Where is the hazard located?What is the hazard?What is the risk (refer Risk Assessment Matrix)?Who is at risk?What action was taken?Further RecommendationsReported by*Referred to*(Workplace Manager or Delegate)Corrective Action Completed Incomplete Interim/short term control(s) requiredLong term control(s) requiredWorkplace Manager's Name:*Δ